
What is Trigger Finger?
Trigger finger, also known as stenosing tenosynovitis, is a common hand condition that affects approximately 2% of the general population and up to 20% of people with diabetes.This condition occurs when smooth flexion and extension of the affected finger is impaired due to a size discrepancy between the flexor tendon (which becomes larger or wider) and the flexor tendon sheath in which it resides (which becomes smaller or narrower).
The condition most frequently affects the ring finger, followed by the thumb, and is more common in women than men, with peak occurrence in the 50s or 60s.
Understanding the Pathophysiology
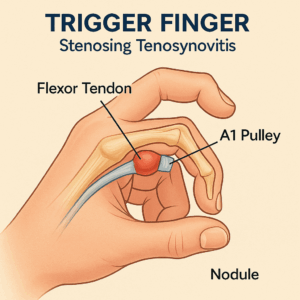
Trigger finger develops when irregular connective tissue and chondrocyte metaplasia cause thickening of both the flexor tendon sheath and the flexor tendon itself, creating a mechanical obstruction at the first annular (A1) pulley during finger movement. Contrary to what the name might suggest, there is typically a lack of inflammatory changes in the affected tissues.
 Figure 2 Overview of Pathophysiology, Diagnosis, and Treatment of Trigger Finger (Stenosing Tenosynovitis) undefined
Figure 2 Overview of Pathophysiology, Diagnosis, and Treatment of Trigger Finger (Stenosing Tenosynovitis) undefined
Risk Factors
Key risk factors for developing trigger finger include:Occupations or activities requiring repetitive gripping or pinching; Diabetes mellitus (prevalence ranges from 4% to 55% in diabetic populations); Age between 40 and 60 years; Female gender; Obesity; Inflammatory arthritis; Metabolic disorders
Clinical Presentation and Diagnosis
Symptoms
Early-stage symptoms include: Subtle pain along the first annular pulley distribution (located in the distal palm at the metacarpal head); Crepitus with range of motion; Palpable tender nodule along the tendon; Finger getting caught in a flexed position requiring manual unlocking
Advanced-stage symptoms include:
– Inability to fully flex or extend the finger
– Locking of the finger in flexion
– Painful popping or clicking with finger movement
– Possible secondary contracture at the proximal interphalangeal joint
Diagnostic Evaluation
Diagnosis is primarily clinical, based on history and physical examination.Clinical examination typically demonstrates:Tenderness and nodularity of the flexor tendon sheath near the palmar A1 pulley; Motion-based catching or locking; Irregular motion or clicking at the proximal interphalangeal joint
Imaging is usually not necessary, but ultrasonography may be considered if the diagnosis is uncertain. Ultrasound findings include flexor tendon thickening or a palmar nodule caused by fascial thickening over the tendon sheath.
Differential Diagnosis
The differential diagnosis includes: Infection; Extensor tendinitis; Arthritis; Dupuytren Disease ; Carpal Tunnel Syndrome
Current Treatment Options
Conservative Management
First-line conservative treatments include:
– Activity Modification: Minimizing repetitive gripping or pinching activities
– Splinting: Fixed metacarpophalangeal joint orthosis in the neutral position, worn at least 8 hours per day. Metacarpophalangeal extension splinting is better tolerated by patients than distal interphalangeal joint extension splints. A 2023 randomized controlled trial found that splinting alone showed no clinically important differences compared to steroid injection in terms of pain reduction and functional improvement up to 1 year.
– NSAIDs and Physical Therapy: While commonly used, a 2021 Cochrane review found that NSAID injections offered little to no benefit over glucocorticoid injection for trigger finger.
Corticosteroid Injection
Corticosteroid injection is a widely used treatment option with the following evidence:
Efficacy:
– A systematic review reported a 57% success rate for symptom resolution; Corticosteroid with lidocaine showed higher symptom resolution compared to lidocaine alone at 4-week follow-up (56% vs 17%)
– Initial success rate of 72%, with 66% and 61% success rates for second and third injections, respectively[1]
Limitations:
– Higher relapse rate (22%) compared to surgical options (0.4%) at 1-12 months follow-up; Less effective in patients with insulin-dependent diabetes; Blood glucose levels can be elevated for 24-48 hours after injection[1]
Surgical Management
Surgical options include open or percutaneous A1 pulley release:
Open Surgical Release:
– 94% symptom resolution rate at 6-12 months; 6% recurrence rate (compared to 38% with steroid injection); Failure rate of 0.55%; Complication rate of 1%
Percutaneous Release:
– Similar efficacy to open release (failure rate 0.56%); May save time and costs; Potential disadvantage of lower visibility in an anatomically complex area with nearby digital nerves and vessels
Indications for Surgery:
– Recurrence after steroid injection; Advanced symptoms (joint stiffness or inability to fully flex or extend); Patient preference; No response after 6 weeks of nonoperative treatment; Patients with insulin-dependent diabetes (may be more clinically and cost-effective as first-line treatment)
Diabetes: Patients with diabetes, particularly those requiring insulin, have lower success rates with corticosteroid injection and may benefit from first-line surgical management.
Multiple digits: People with diabetes often have multiple affected digits, with prevalence ranging from 4% to 55%.
Pediatric patients: Children are often treated more conservatively with splinting, as trigger finger in children may indicate anatomic variations or inherited conditions.
Prognosis and Outcomes
Most cases of trigger finger respond well to conservative care. Surgical release provides the highest success rate (94%) and lowest recurrence rate (6%). Combining splinting with steroid injection offers no additional benefit over either treatment alone.
Conclusion
Trigger finger is a common, treatable condition with multiple management options. Current evidence supports a stepwise approach beginning with conservative management (activity modification and splinting) for early-stage disease, progressing to corticosteroid injection for persistent symptoms, and ultimately surgical release for refractory cases or advanced disease. Patient-specific factors, particularly diabetes status, should guide treatment selection.
Why Choose Dr. Chambers for Hand and Wrist Care
At Raleigh Orthopaedic Clinic, Dr. Stephen Chambers specializes in hand and upper extremity surgery. With years of expertise in treating hand and wrist injuries, including Trigger Finger, Dr. Chambers provides comprehensive care—ranging from at home treatments and injections to advanced hand surgery when needed. Patients trust Dr. Chambers and his team for personalized care, effective treatment options, and excellent outcomes and describe Dr. Chambers as a caring, attentive, and skilled surgeon with excellent bedside manner. His amazing team ensures every patient feels supported and informed throughout the process.
If you are experiencing wrist pain, swelling, or difficulty with wrist movements, don’t wait for symptoms to worsen. Schedule an Appointment with Dr. Chambers today to Trigger Finger and get back to normal use of your hand . Experience the benefit of specialized hand care close to home at Raleigh Orthopaedics in Raleigh, Cary, Holly Springs, and Wake Forest, North Carolina