
Wrist Ligament Injury Treatment in Raleigh, NC
Wrist pain after a fall, a persistent click with wrist motion, or a feeling of instability? Wrist ligament injuries — especially the scapholunate ligament — are a leading cause of chronic wrist pain that progresses to arthritis if not properly treated.
What Is Wrist Ligament Injury?
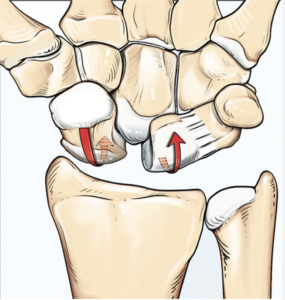
The wrist contains eight carpal bones linked by a complex system of intrinsic and extrinsic ligaments. The scapholunate (SL) ligament — connecting the scaphoid and lunate — is the most clinically important. SL ligament tears cause abnormal carpal mechanics that lead, predictably, to SLAC (Scapholunate Advanced Collapse) wrist arthritis over years to decades.
The lunotriquetral (LT) ligament on the ulnar side is the second most commonly injured intrinsic ligament. Both can occur from the same fall mechanism as TFCC tears — making careful examination of all structures essential.
ⓘ An untreated complete SL ligament tear will almost certainly lead to SLAC wrist arthritis over 5–20 years. Early repair — within 3–6 weeks of injury — is technically much simpler and produces better outcomes than reconstruction of a chronic tear.
Risk Factors
Several factors increase the likelihood of developing this condition.
Fall on Outstretched Hand
FOOSH — the classic mechanism
Snowboarding / Skiing
Wrist guards help but falls still injure ligaments
Gymnastics
Wrist loading and falls
Contact Sports
Wrestling and grappling injuries
Weightlifting
Axial wrist loading
Racquet Sports
Wrist torque during strokes
Stages of Wrist Ligament Injury
Ligament stretched or partially torn. Carpal alignment maintained.
Complete SL tear within 6 weeks. Carpal instability present. Best repair window.
Chronic complete tear with carpal collapse. Complex reconstruction needed.
Diagnosis
The Watson test (scaphoid shift test) provokes a painful clunk as the scaphoid subluxes — highly specific for SL instability. MRI arthrogram with contrast confirms the tear. Wrist arthroscopy is the gold standard, allowing direct ligament assessment and classification (Geissler Grade I–IV).
- ✓Watson test (scaphoid shift)
- ✓Lunotriquetral shear test
- ✓MRI arthrogram (3T preferred)
- ✓X-rays (PA with clenched fist, lateral for DISI deformity)
- ✓Wrist arthroscopy (gold standard)
- ✓Geissler arthroscopic grading
Treatment Outcomes & Statistics
Published outcome data to help you make an informed decision.
Grade I–II partial tears respond well to immobilization and therapy
Acute complete SL repair within 6 weeks — excellent outcomes
Tendon graft reconstruction for chronic tears — reasonable but limited outcomes
Virtually all untreated complete SL tears develop SLAC arthritis over 10–20 years
Complication Profile
| Complication | Rate | Severity | Notes |
|---|---|---|---|
| SLAC arthritis (untreated) | ~100% over time | Serious | Predictable arthritis from untreated complete SL tear |
| Wrist stiffness | 15–20% | Moderate | Common after ligament repair and immobilization |
| Failed reconstruction | 20–30% | Moderate | Chronic SL reconstruction — reasonable but not guaranteed |
| Infection | <1% | Minor | Very rare |
Source: Larsen et al., J Hand Surg; Short et al., J Hand Surg; Watson & Ballet
Treatment Options
Dr. Chambers will recommend the best approach based on your severity, goals, and lifestyle.
Immobilization & Therapy (Partial Tears)
Grade I–II partial SL ligament tears heal well with 6 weeks of cast immobilization. Proprioceptive training and wrist strengthening follow. Arthroscopic thermal shrinkage is an option for Grade II tears not responding to casting.
Acute SL Ligament Repair
Within 6 weeks of complete injury, the ligament ends can be repaired directly with suture anchors and protected with K-wires across the SL joint. This is the simplest and most successful surgery for SL injuries — strongly favoring prompt evaluation.
Chronic SL Reconstruction
Chronic complete tears require tendon graft reconstruction — replacing the torn ligament with a strip of the flexor carpi radialis tendon woven through bone tunnels. More complex surgery with more variable outcomes than acute repair.
What to Expect During Recovery
Immobilization
Cast with K-wires (if placed). Fingers kept moving. No wrist use.
K-wire Removal & Motion
K-wires removed at 8–10 weeks. Wrist range-of-motion exercises begin. Dynamic splint if stiff.
Strengthening
Progressive wrist strengthening. Return to most daily activities. Sport-specific training.
Full Return
Return to sport and manual work. Serial X-rays monitor carpal alignment.
Frequently Asked Questions
A wrist sprain is a broad term including minor ligament strains that heal fully within weeks. A scapholunate ligament tear is a specific structural injury to the most important carpal ligament — which, if complete and untreated, virtually always leads to SLAC wrist arthritis over years. Persistent wrist pain beyond 6 weeks after a "sprain" warrants specialist evaluation and MRI.
An acute complete SL tear can be repaired directly within 6 weeks — a relatively simple, highly successful procedure. After 6 weeks, the ligament ends retract and scar down, making primary repair impossible. Reconstruction with a tendon graft is more complex and has significantly lower success rates. Waiting weeks or months because symptoms seem "minor" is the most common reason for poor outcomes.
A partial tear properly treated will not cause arthritis. An untreated complete SL tear will — virtually predictably — develop SLAC arthritis over 10–20 years. This is why complete SL tears in young and active patients should be treated promptly, even if symptoms seem manageable in the short term.
Wrist Instability or Clicking After a Fall?
Wrist ligament injuries are time-sensitive. Early evaluation gives the best treatment options. No referral needed.

Stephen Chambers, M.D.
Dual Board-Certified Hand & Upper Extremity Surgeon · Raleigh Orthopaedic









