
Fingertip Amputation Treatment in Raleigh, NC
A fingertip injury from a saw, door, or lawn mower is frightening. Many fingertip amputations can be managed without replantation — achieving excellent cosmetic and functional results, especially in children.
What Is Fingertip Amputation?
Fingertip amputations are classified by zone: Zone I (soft tissue only, distal to the bone tip), Zone II (bone exposed or shortened), and Zone III (through or proximal to the DIP joint). Treatment depends on zone, patient age, occupation, which finger is involved, and the condition of the amputated part.
Options include conservative wound healing, skin grafting, local flap reconstruction, or replantation. Interestingly, Zone I amputations — especially in children — often do better with conservative management than with complex surgery.
ⓘ If there is an amputated part: wrap it in moist gauze, place in a clean bag, and put the bag on ice (not directly in ice). Bring it to the appointment — Dr. Chambers will assess whether replantation is appropriate.
Risk Factors
Several factors are associated with a higher likelihood of developing this condition.
Power Tools
Saw, drill, lathe, grinder
Home Accidents
Kitchen tools, door hinges
Lawn Equipment
Mowers, trimmers, edgers
Industrial Machinery
Crush and avulsion injuries
Children
Doors, bicycle spokes (very common)
Sharp Objects
Knife and cutting board injuries
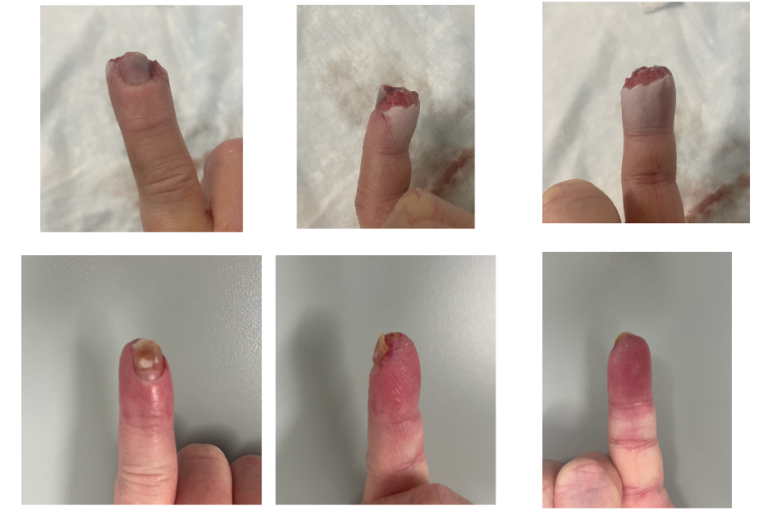
Stages of Fingertip Amputation
Skin and fat loss distal to the bone tip. Excellent healing capacity.
Soft tissue loss with bone exposure or requiring shortening.
Amputation at or proximal to the DIP joint. Replantation evaluation indicated.
Diagnosis
Dr. Chambers examines the wound zone, the amputated part if available, X-rays to assess bone level, and factors including the patient's occupation, dominant hand, and functional needs. The decision between conservative management, flap coverage, graft, or replantation requires specialist evaluation.
- ✓Zone classification of amputation level
- ✓X-rays of injury and amputated part (if present)
- ✓Assessment of amputated part viability
- ✓Vascular status (bleeding, capillary refill)
- ✓Patient occupation, hand dominance, and functional needs
Treatment Outcomes & Statistics
Published outcome data to help you make an informed decision. Dr. Chambers will review what these numbers mean for your specific case at your visit.
Zone I injuries achieve very good to excellent outcomes with wound care alone
Fingertip replantation survival at specialized centers
Replanted fingers achieve useful function — not always better than stump
Typical healing time for Zone I with conservative management
Complication Profile
| Complication | Rate | Severity | Notes |
|---|---|---|---|
| Cold intolerance | 60–80% replants | Moderate | Very common after replantation; usually improves over years |
| Hook nail deformity | 10–20% | Moderate | After certain flap reconstructions; usually minor |
| Hypersensitivity | Common | Moderate | Managed with desensitization exercises |
| Replant failure | 20% of replants | Serious | Requires revision amputation |
Source: Rosberg et al., Acta Orthop; Sebastin & Chung, J Hand Surg
Treatment Options
Dr. Chambers will recommend the best approach based on your severity, goals, and lifestyle. Most conditions are first treated non-surgically.
Wound Healing (Secondary Intention)
Zone I amputations — especially in children — heal remarkably well with moist wound care and time. The fingertip has excellent regenerative capacity. This avoids surgery and often achieves near-normal appearance with preserved sensation.
Skin Graft or Local Flap
For larger defects, exposed bone, or Zone II injuries, a skin graft from the forearm or a local finger flap provides coverage while preserving finger length. Multiple flap techniques are available (V-Y, thenar, cross-finger).
Replantation
Microsurgical reattachment of the amputated part — arteries, veins, nerves, and tendons repaired. Best for clean amputations in young, healthy patients. Not always the best option — replanted fingertips can be cold, stiff, and painful.
What to Expect During Recovery
Wound Management
Daily dressing changes. Keep elevated. Infection prevention. Protective fingertip splint.
Healing Phase
Wound contracts and epithelializes. Sensation begins to return. Protective splint as needed.
Scar Maturation & Desensitization
Fingertip contour improving. Desensitization exercises for hypersensitivity. Scar massage.
Return to Activity
Full return to work and activities. Sensation recovery continues — especially in younger patients.
Frequently Asked Questions
Always bring the amputated part — wrap in moist gauze, in a bag, on ice. Dr. Chambers will assess whether replantation is appropriate. For Zone I (fingertip-level) amputations, conservative management often achieves better or equivalent results than replantation with less recovery time. Replantation is more strongly indicated for thumb amputations, more proximal injuries, and in children.
With conservative management, sensation often recovers remarkably well — especially in younger patients and children. Nerve regeneration proceeds at about 1mm per day from the nearest intact nerve ending. Full recovery may take months but is often near-normal for Zone I injuries.
Yes — children under approximately 12 years old have remarkable fingertip regenerative capacity. Zone I amputations in children frequently heal almost perfectly with conservative wound care alone — including near-complete restoration of the fingertip contour, nail, and sensation.
Dr. Chambers will give you detailed dressing change instructions. In general: keep the wound clean and moist with appropriate dressings, keep the finger elevated for the first few days, and protect it from additional injury with a fingertip guard. Warm soaks begin when the wound has adequately closed.
Fingertip Injury? Expert Evaluation Today.
Outcomes depend on proper early management. Same-week appointments available. No referral needed.

Stephen Chambers, M.D.
Dual Board-Certified Hand & Upper Extremity Surgeon · Raleigh Orthopaedic