
Hand Fractures Treatment in Raleigh, NC
Broken a bone in your hand? Hand fractures are among the most common injuries Dr. Chambers treats. Prompt evaluation ensures bones heal in proper alignment — preventing permanent stiffness, deformity, or arthritis.
What Is Hand Fractures?
Hand fractures involve breaks in the metacarpal bones (the five bones in the middle of the hand connecting to the knuckles) or the phalanges (the finger bones). The most common metacarpal fracture is the 'Boxer's fracture' — a break at the neck of the small finger metacarpal from a punch.
The goal of treatment — surgical or not — is to restore proper bone alignment so the hand can make a full fist and fingers don't rotate or overlap during grip. Even mild rotational deformity can cause significant functional problems.
ⓘ Never ignore a hand fracture. A finger that heals even slightly rotated can cause fingers to overlap during grip — a deformity that is much harder to correct months later.
Risk Factors
Several factors are associated with a higher likelihood of developing this condition.
Sports Injury
Punching, blocking, ball impact
Fall
Landing on outstretched hand
Crush
Door, machinery, or industrial trauma
Workplace
Industrial and manual labor
Ball Sports
Baseball, basketball, volleyball
Punch
Boxer's fracture — 5th metacarpal neck
Stages of Hand Fractures
Bone broken but properly aligned. Splinting is usually sufficient for healing.
Bone out of alignment. May need reduction (manipulation) with or without surgery.
Fracture into a joint, multiple fragments, or open fracture with skin break.
Diagnosis
Dr. Chambers evaluates hand fractures with X-rays in multiple views (AP, lateral, oblique). CT scan is occasionally needed for complex articular fractures. Rotational alignment is assessed clinically — you'll be asked to make a fist. All fingers should point toward the same spot (the scaphoid). Overlapping fingers indicate rotation.
- ✓X-rays (AP, lateral, oblique views)
- ✓Rotational alignment assessment — fist view
- ✓Skin assessment for open fracture
- ✓Neurovascular exam (circulation and sensation)
- ✓CT scan if articular fracture suspected
Treatment Outcomes & Statistics
Published outcome data to help you make an informed decision. Dr. Chambers will review what these numbers mean for your specific case at your visit.
Stable fractures heal very well with splinting alone
Good bone alignment achieved with appropriate treatment
Most hand fractures heal sufficiently in 3–6 weeks
Very low rate of poor alignment with appropriate management
Complication Profile
| Complication | Rate | Severity | Notes |
|---|---|---|---|
| Stiffness / reduced grip | 15–25% | Moderate | Hand therapy is key; most improve fully with time |
| Malunion (poor alignment) | <5% | Serious | Prevented with close follow-up and proper splinting |
| Infection (open fractures) | 2–5% | Moderate | Antibiotics and washout; higher risk with contamination |
| Hardware irritation (if surgery) | 5–10% | Minor | Screws or plates occasionally removed after healing |
Source: ASSH Hand Fracture Guidelines; Page & Stern, Hand Clin 2010
Treatment Options
Dr. Chambers will recommend the best approach based on your severity, goals, and lifestyle. Most conditions are first treated non-surgically.
Splinting / Buddy Taping
Stable, well-aligned fractures are treated with an appropriate splint or cast for 3–4 weeks. Buddy taping to the adjacent finger helps control rotation in finger fractures while allowing early motion.
Closed Reduction
Displaced fractures are manipulated back into alignment under local or regional anesthesia, then held in a splint. No incision required. Successful in many cases and avoids surgery entirely.
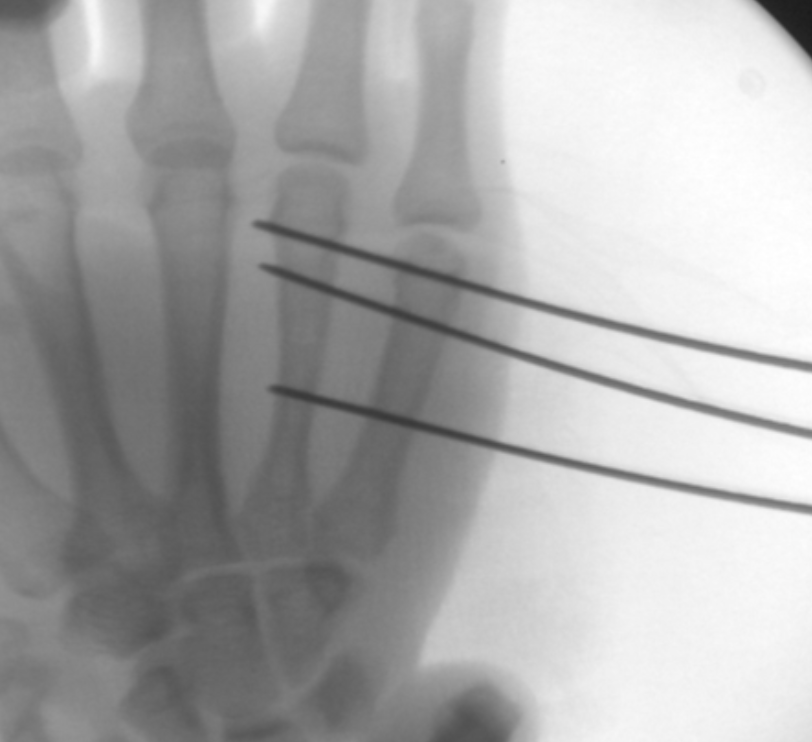
ORIF / Pinning (K-wires or Screws/Plates)
Open reduction with screws, plates, or K-wires for unstable, rotated, articular, or irreducible fractures. Restores anatomy precisely and allows earlier motion rehabilitation.
What to Expect During Recovery
Immobilization
Splint or cast immobilization. Elevation reduces swelling. Shoulder and elbow kept moving to prevent stiffness.
Fracture Check
Repeat X-rays confirm healing and alignment. Most patients begin range-of-motion exercises.
Motion Recovery
Gradual return to full fist. Hand therapy if stiffness. Buddy taping for return to sports.
Full Activity
Full grip strength and activity resumed. Hand therapy for complex fractures continues as needed.
Frequently Asked Questions
About 70% of hand fractures are treated non-surgically with splinting. Surgery is recommended when the bone is significantly displaced, rotated, extends into a joint, or when closed reduction cannot hold alignment. Dr. Chambers will give you a clear recommendation after reviewing your X-rays.
A Boxer's fracture is a break at the neck of the 5th metacarpal (small finger knuckle), most often from punching. Despite the name, it often heals very well with splinting alone. Surgery is reserved for significant angulation (>40°) or rotational deformity.
Finger fractures typically allow light hand use by 4–6 weeks. Metacarpal fractures are usually healed enough for full use by 6–8 weeks. Complex articular or surgically treated fractures may take 8–12 weeks before full grip activities.
Most patients benefit significantly from hand therapy after a fracture — especially to prevent stiffness, which is the most common long-term problem. Dr. Chambers will refer you to an occupational hand therapist when appropriate.
Hand Fracture? Get Evaluated Today.
Proper alignment is critical for long-term function. No referral needed — same-week appointments at all Triangle locations.

Stephen Chambers, M.D.
Dual Board-Certified Hand & Upper Extremity Surgeon · Raleigh Orthopaedic
Below are examples of surgical treatment options. Each depend on the fracture type.


Click Here for More Information