
Wrist Sprain & TFCC Tear Treatment in Raleigh, NC
Wrist pain on the pinky side after a fall or twist? Persistent pain that won't go away after a "sprain"? You may have a TFCC tear — the most common cause of ulnar-sided wrist pain — and one of the most underdiagnosed wrist injuries.
What Is Wrist Sprain & TFCC Tear?
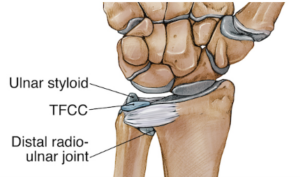
The triangular fibrocartilage complex (TFCC) is a cartilage structure on the ulnar (pinky) side of the wrist that stabilizes the distal radioulnar joint and cushions the ulnar side of the carpus. It acts as the wrist's meniscus. TFCC tears are classified as Type I (traumatic — from a fall or twist) or Type II (degenerative — wear-related, associated with a long ulna).
Simple wrist sprains without TFCC injury typically heal within 4–6 weeks. Persistent ulnar-sided pain beyond 6 weeks after injury should raise suspicion for a TFCC tear, which requires specific diagnosis and management.
ⓘ Ulnar-sided wrist pain lasting more than 6 weeks after injury is not just a sprain. TFCC tears, lunotriquetral ligament injuries, and ECU tendon problems are common causes that require specialist evaluation.
Risk Factors
Several factors increase the likelihood of developing this condition.
Fall on Outstretched Hand
Most common traumatic cause
Forearm Rotation Injury
Pronation/supination force at wrist
Racquet Sports
Racquet handle torque during swing
Weightlifting
Axial loading during lifts
Positive Ulnar Variance
Long ulna predisposes to Type II degenerative tears
Age 40+
Degenerative Type II tears more common
Stages of Wrist Sprain & TFCC Tear
Traumatic tear at the vascular periphery — good healing potential.
Traumatic central tear — avascular zone, poor healing potential.
Wear-related tear associated with ulnar impaction. May require ulnar shortening.
Diagnosis
TFCC tears are diagnosed with clinical tests (TFCC compression test, ulnocarpal stress test) combined with MRI. Wrist arthroscopy remains the gold standard — it allows direct visualization and simultaneous treatment. Dr. Chambers assesses ulnar variance on X-rays to determine if ulnar shortening is needed.
- ✓TFCC compression test (axial load + ulnar deviation)
- ✓Ulnocarpal stress test
- ✓Piano key test (DRUJ instability)
- ✓MRI (preferably 3T with arthrogram for best detail)
- ✓X-rays for ulnar variance measurement
- ✓Wrist arthroscopy (gold standard diagnosis and treatment)
Treatment Outcomes & Statistics
Published outcome data to help you make an informed decision.
Type Ib peripheral tears respond well to 4–6 weeks immobilization
Short arm cast or splint in neutral forearm rotation
Central tears less likely to fully resolve — may need debridement
Corticosteroid injection into DRUJ provides meaningful pain relief
Complication Profile
| Complication | Rate | Severity | Notes |
|---|---|---|---|
| Residual pain | 20–30% | Moderate | Common with central tears — may need arthroscopy |
| Stiffness | 15% | Minor | Forearm rotation restriction; addressed with therapy |
| DRUJ instability | Variable | Moderate | May persist with complete peripheral tears requiring repair |
Source: Hermansdorfer & Kleinman, J Hand Surg 1991; Luchetti et al., Arthroscopy 1996
After arthroscopic repair or debridement
Peripheral tears with good vascularity — excellent healing
Central tears — pain relief with arthroscopic debridement
Most athletes return within 3 months of repair
Complication Profile
| Complication | Rate | Severity | Notes |
|---|---|---|---|
| Stiffness | 10–15% | Minor | Addressed with therapy |
| Portal site complications | <2% | Minor | Infection or nerve irritation — rare |
| Re-tear | 5–10% | Moderate | Lower rate with peripheral repairs in vascular zone |
| Incomplete pain relief | 10–15% | Moderate | Central tears may have residual symptoms |
Source: Minami et al., J Hand Surg 1996; Estrella et al., J Hand Surg 2007
Treatment Options
Dr. Chambers will recommend the best approach based on your severity, goals, and lifestyle.
Cast / Splint Immobilization
4–6 weeks in a short arm cast or splint in neutral forearm rotation gives peripheral TFCC tears the best chance to heal. This is the preferred initial treatment for acute Type I tears. Most patients with peripheral tears heal well.
Cortisone Injection into DRUJ
A corticosteroid injection into the distal radioulnar joint provides meaningful short-term pain relief and helps confirm the source of pain. Useful for Type II degenerative tears and as a temporizing measure.
Wrist Arthroscopy (Repair or Debridement)
Arthroscopic surgery allows direct visualization and treatment. Peripheral tears are repaired with sutures; central tears are debrided (trimmed). Type II degenerative tears may additionally require ulnar shortening osteotomy to address the root cause.
What to Expect During Recovery
Immobilization
Cast or splint. Protect the TFCC while initial healing occurs. Shoulder and elbow exercises maintained.
Motion Recovery
Cast removed. Forearm rotation exercises begin. Gradual return to daily activities.
Strengthening
Progressive grip and forearm strengthening. Return to most activities without heavy loading.
Full Return
Return to sport and manual work. Full forearm rotation and grip strength restored.
Frequently Asked Questions
Simple wrist sprains typically resolve within 4–6 weeks with rest. If you have persistent pain specifically on the pinky side of the wrist — especially with forearm rotation like turning a doorknob or key — beyond 6 weeks after injury, a TFCC tear is likely. Dr. Chambers will perform clinical tests and order an MRI to confirm.
Peripheral (outer edge) tears have a good blood supply and 80% heal with 4–6 weeks of cast immobilization. Central tears are in an avascular zone and do not heal on their own — arthroscopic debridement removes the torn tissue and reduces pain. Whether you need surgery depends on the tear type, location, and your response to conservative treatment.
Ulnar variance refers to the relative length of the ulna compared to the radius. Positive ulnar variance means the ulna is longer than average — this causes the ulna to impact the TFCC and carpal bones with every wrist movement (ulnar impaction syndrome). It is the main cause of Type II degenerative TFCC tears, and ulnar shortening osteotomy addresses the root cause.
Most patients return to light activities within 2–4 weeks and to sport by 3–6 months. Peripheral TFCC repairs require 4–6 weeks of immobilization followed by gradual rehabilitation. Recovery from ulnar shortening osteotomy takes longer — typically 4–6 months.
Pinky-Side Wrist Pain That Won't Go Away?
TFCC tears are commonly missed as "sprains." Get an accurate diagnosis. No referral needed.

Stephen Chambers, M.D.
Dual Board-Certified Hand & Upper Extremity Surgeon · Raleigh Orthopaedic









